

Abstract
Introduction: A hallmark of Multiple Myeloma (MM) is the sequel development of drug resistant phenotypes, which may be present initially or emerge during the course of treatment. These drug resistant phenotypes reflect the intra-tumor and inter-patient heterogeneity of this cancer. Most MM cells are sensitive to proteasome inhibitors (PIs), which have become the standard of care in the treatment of newly diagnosed and relapsed MM. However, resistance develops (intrinsic/acquired). Although several novel drugs have recently been approved or are in development for MM, there are few molecular indicators to guide treatment selection. To address this limitation we have combined mass spectrometry-based proteomics analysis together with ex vivo drug response profiles and clinical outcome to elucidate a best possible accurate phenotype of the resistant sub-clones, thus yielding a theranostic profile that will inform therapeutic and drug development strategies.
Methods: We performed mass spectrometry-based proteomics analysis on plasma cells isolated from 38 adult MM patient bone marrow aspirates (CD138+). Samples were obtained at diagnosis or prior to commencing therapy. The participating subjects gave written informed consent in accordance with the Declaration of Helsinki that was approved by local ethics committees. For the proteomics analysis, peptides were purified using the filtered aided sample preparation (FASP) method. Subsequently, samples were prepared for label-free liquid chromatography mass spectrometry (LC-MS/MS) using a Thermo Scientific Q-Exactive MS mass spectrometer. Proteins were analysed using the MaxQuant and Perseus software for mass-spectrometry (MS)-based proteomics data analysis, UniProtKB-Swiss Prot database and KEGG Pathway database. In parallel, we undertook a comprehensive functional strategy to directly determine the drug dependency of myeloma plasma cells based on ex vivo drug sensitivity and resistance testing (DSRT)as previously described (1).
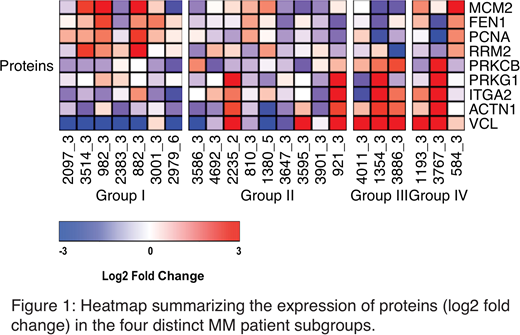
Results: Our initial proteomic analysis was generated by examining MM patient plasma cells, grouped based on DSRT to 142 anticancer drugs including standard of care and investigational drugs. Each of the 142 drugs was tested over a 10,000-fold concentration range, allowing for the establishment of accurate dose-response curves for each drug in each patient. MM patients were stratified into four distinct subgroups as follows: highly sensitive (Group I), sensitive (Group II), resistant (Group III) or highly resistant (Group IV) to the panel of drugs tested. We then performed blinded analysis on the 4 groups of CD138+ plasma cells divided based on the ex vivo sensitivity profile, identifying a highly significant differential proteomic signature between the 4-chemosensitivity profiles, with Cell Adhesion Mediated-Drug Resistance (CAM-DR) related proteins (e.g. integrins αIIb and β3) significantly elevated in the highly resistant phenotype (Group IV). In addition our results showed that Group I patients displayed significant upregulation of cell proliferation proteins including: MCM2, FEN1, PCNA and RRM2. Furthermore, Group I patients have shorter Progression Free Survival (PFS) as well as Overall Survival (OS) compared to the other subgroups. Figure 1 shows the Heatmap summarizing the expression of proteins (log2 fold change) in the four distinct MM patient subgroups.
Conclusions:Our findings suggest that combining a proteomics based study together with drug sensitivity and resistance testing allows for an iterative adjustment of therapies for patients with MM, one patient at a time, thus providing a theranostic approach. Our results suggest that the disease driving mechanisms in the patient subgroups are distinct, with highly resistant patients exhibiting cell adhesion mediated cytoprotection, while highly sensitive patients show an increased cell proliferation protein profile with shorter PFS and OS. Our study aims to guide treatment decisions for individual cancer patients coupled with monitoring of subsequent responses in patients to measure and understand the efficacy and mechanism of action of the drugs. Future work will include the establishment of flow cytometry-based screening assays to identify the different resistant phenotypes at diagnosis/relapse.
References: (1) M. M. Majumder et al., Oncotarget 8(34), 56338 (2017)
Anttila:Amgen: Membership on an entity's Board of Directors or advisory committees; Takeda: Consultancy, Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees. Silvennoinen:Amgen: Honoraria, Research Funding; Takeda: Honoraria, Research Funding; Celgene: Honoraria, Research Funding; BMS: Honoraria, Research Funding. Heckman:Orion Pharma: Research Funding; Celgene: Research Funding; Novartis: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal